Oct. 30, Mon, 2023
Topics
>RESEARCH
Shedding Light on the Paradoxical Prognosis for Patients with Cardiac Sarcoidosis, a Rare and Difficult-to-Diagnose Inflammatory Heart Condition
Scientists run statistical analyses on large cohort to clarify why prognosis seems to be worse when sarcoidosis is confined exclusively to the heart
While cardiac sarcoidosis (CS) tends to be systemic and affects multiple organs, existing literature suggests that prognosis is worse for patients with isolated CS, which affects only the heart. In a recent study, researchers from Japan delve into this puzzling issue and conduct secondary statistical analyses on one of the largest CS cohorts. Their findings highlight the importance of a patient’s condition at the time of diagnosis as well as the early detection of CS.
The paradoxical prognosis for patients with cardiac sarcoidosis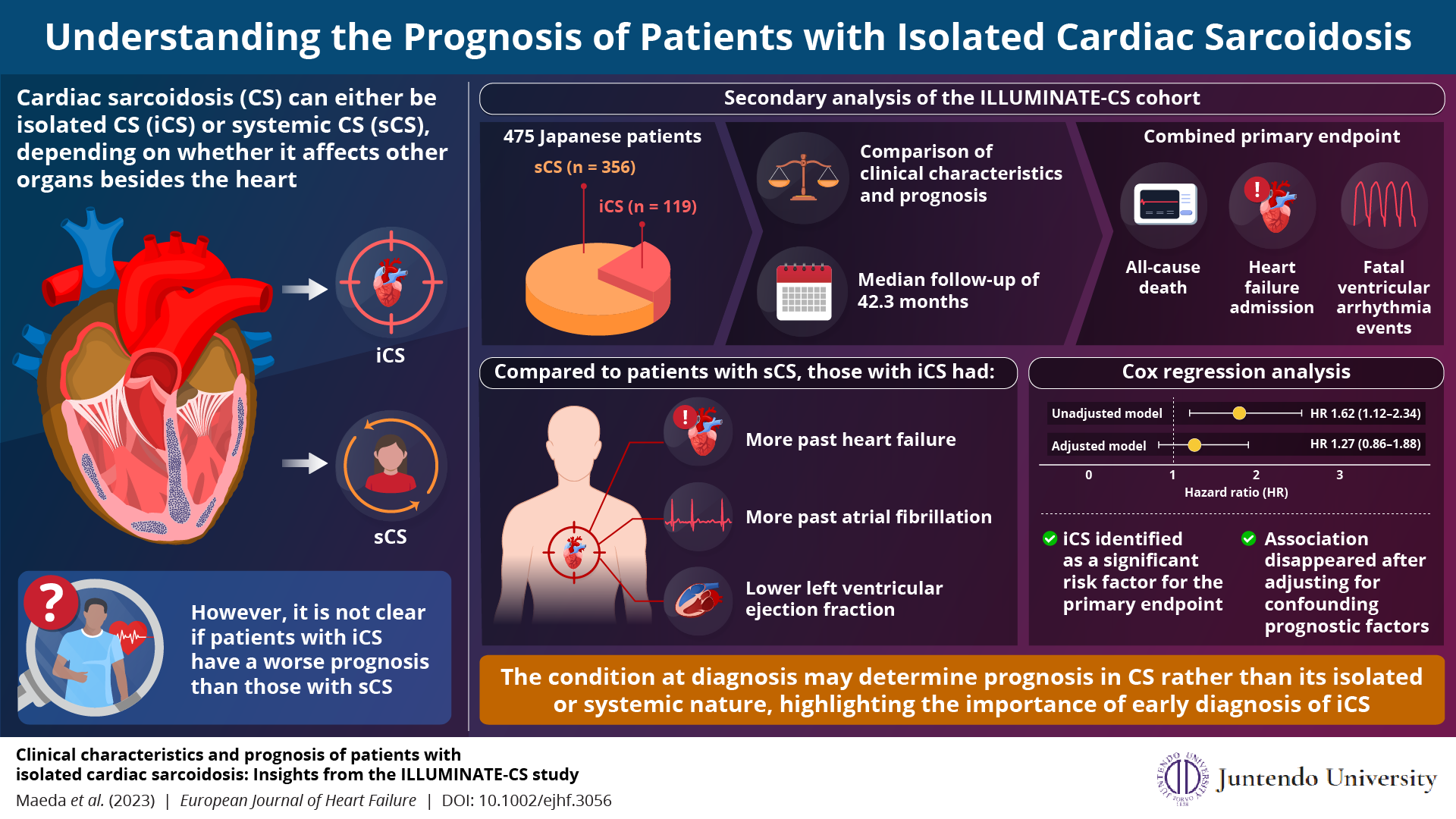
The paradoxical prognosis for patients with cardiac sarcoidosis
Researchers investigate why patients with isolated cardiac sarcoidosis seem to have a worse prognosis than those with systemic cardiac sarcoidosis, highlighting the importance of early diagnosis.
Image Credit:Dr. Daichi Maeda from Juntendo University, Japan
License type:Original Content
Usage restrictions: You are free to share and adapt the Infographic material but attribution is required, with a link to the news source.
Image Credit:Dr. Daichi Maeda from Juntendo University, Japan
License type:Original Content
Usage restrictions: You are free to share and adapt the Infographic material but attribution is required, with a link to the news source.
Sarcoidosis is a complex inflammatory disease that causes the harmful accumulation of tiny clumps of cells called granulomas in the body. In most cases, sarcoidosis manifests in the lungs and lymph nodes. However, in approximately 10% of patients, the heart is affected; this condition is known as ‘cardiac sarcoidosis (CS).’ Although relatively rare, CS can cause life-threatening complications, including arrhythmia, heart failure, or sudden cardiac death.
One puzzling aspect of CS is that the condition sometimes involves the heart alone, without manifesting clinically apparent symptoms in other organs. This is referred to as isolated CS (iCS), in contrast to the multi-organ condition called systemic CS (sCS). According to previous studies, patients diagnosed with iCS have a poorer prognosis than those with sCS, despite the latter condition involving multiple organs instead of just the heart.
This seemingly paradoxical finding prompted a research team to investigate the issue in greater detail. The researchers, led by Assistant Professor Daichi Maeda of the Department of Cardiovascular Biology and Medicine at the Juntendo University Graduate School of Medicine, Japan recently conducted detailed statistical analyses to explain the above findings. Their study, published in the European Journal of Heart Failure on October 12th, 2023, is co-authored by Yuya Matsue and Tohru Minamino of Juntendo University, among others.
The team obtained the data for this study from the ‘ILLUstration of the Management and prognosIs of JapaNese pATiEnts with Cardiac Sarcoidosis (ILLUMINATE-CS)’ cohort, a large multicenter, retrospective cohort database. They compared the prognosis and selected clinical characteristics from among a total of 475 patients with iCS or sCS. The primary outcome was a combined endpoint including all-cause death, hospitalization for heart failure, and fatal ventricular arrhythmia events.
The analysis revealed that patients with iCS were more likely to have a history of atrial fibrillation or heart failure than those with sCS, as well as a lower ventricular ejection fraction (LVEF) and thus more impaired heart function. According to a Cox proportional hazard analysis using an unadjusted model, patients with iCS were more likely to have a worse prognosis than patients with sCS based on the defined primary outcome. However, this association vanished when the model was adjusted for other confounding factors.
These results have important implications, as Dr. Maeda explains: “Our findings suggest that the conditions at the time of diagnosis determine a patient’s prognosis rather than whether they have iCS or sCS. Therefore, the early detection of iCS is critical, although there are fewer opportunities to suspect the disease before symptoms appear.” He further adds that once a patient exhibits decreased LVEF or experiences cardiac events, the possibility of CS should be investigated so that they can be treated with immunosuppressors. Notably, this study also found that both patients with iCS and sCS responded equally well to steroid treatment.
Overall, this work sheds valuable light on some intriguing aspects of CS and highlights the need for further investigation. “We hope that our current study facilitates the development of an early diagnostic tool for CS and that researchers around the world engage in studies on CS,” concludes Dr. Maeda.
We envision a future where all types of sarcoidosis can be timely diagnosed and managed.
About Assistant Professor Daichi Maeda from Juntendo University
Dr. Daichi Maeda obtained his PhD from Osaka Medical College, Japan, in 2020, where he also served as Assistant Professor for a year. In April 2021, he joined the Department of Cardiovascular Biology and Medicine at Juntendo University, where he currently serves as Assistant Professor. His research focuses on heart failure and cardiomyopathies. He has over 50 publications to his name on these topics. He is also a member of the Japanese Circulation Society and the Japanese Heart Failure Society.
One puzzling aspect of CS is that the condition sometimes involves the heart alone, without manifesting clinically apparent symptoms in other organs. This is referred to as isolated CS (iCS), in contrast to the multi-organ condition called systemic CS (sCS). According to previous studies, patients diagnosed with iCS have a poorer prognosis than those with sCS, despite the latter condition involving multiple organs instead of just the heart.
This seemingly paradoxical finding prompted a research team to investigate the issue in greater detail. The researchers, led by Assistant Professor Daichi Maeda of the Department of Cardiovascular Biology and Medicine at the Juntendo University Graduate School of Medicine, Japan recently conducted detailed statistical analyses to explain the above findings. Their study, published in the European Journal of Heart Failure on October 12th, 2023, is co-authored by Yuya Matsue and Tohru Minamino of Juntendo University, among others.
The team obtained the data for this study from the ‘ILLUstration of the Management and prognosIs of JapaNese pATiEnts with Cardiac Sarcoidosis (ILLUMINATE-CS)’ cohort, a large multicenter, retrospective cohort database. They compared the prognosis and selected clinical characteristics from among a total of 475 patients with iCS or sCS. The primary outcome was a combined endpoint including all-cause death, hospitalization for heart failure, and fatal ventricular arrhythmia events.
The analysis revealed that patients with iCS were more likely to have a history of atrial fibrillation or heart failure than those with sCS, as well as a lower ventricular ejection fraction (LVEF) and thus more impaired heart function. According to a Cox proportional hazard analysis using an unadjusted model, patients with iCS were more likely to have a worse prognosis than patients with sCS based on the defined primary outcome. However, this association vanished when the model was adjusted for other confounding factors.
These results have important implications, as Dr. Maeda explains: “Our findings suggest that the conditions at the time of diagnosis determine a patient’s prognosis rather than whether they have iCS or sCS. Therefore, the early detection of iCS is critical, although there are fewer opportunities to suspect the disease before symptoms appear.” He further adds that once a patient exhibits decreased LVEF or experiences cardiac events, the possibility of CS should be investigated so that they can be treated with immunosuppressors. Notably, this study also found that both patients with iCS and sCS responded equally well to steroid treatment.
Overall, this work sheds valuable light on some intriguing aspects of CS and highlights the need for further investigation. “We hope that our current study facilitates the development of an early diagnostic tool for CS and that researchers around the world engage in studies on CS,” concludes Dr. Maeda.
We envision a future where all types of sarcoidosis can be timely diagnosed and managed.
About Assistant Professor Daichi Maeda from Juntendo University
Dr. Daichi Maeda obtained his PhD from Osaka Medical College, Japan, in 2020, where he also served as Assistant Professor for a year. In April 2021, he joined the Department of Cardiovascular Biology and Medicine at Juntendo University, where he currently serves as Assistant Professor. His research focuses on heart failure and cardiomyopathies. He has over 50 publications to his name on these topics. He is also a member of the Japanese Circulation Society and the Japanese Heart Failure Society.
Reference
| Authors | Daichi Maedaa, Yuya Matsuea, Taishi Dotarea, Tsutomu Sunayamaa, Takashi Isoa, Kenji Yoshiokab, Takeru Nabetac,d, Yoshihisa Narusee, Takeshi Kitaif, Tatsunori Taniguchig, Hidekazu Tanakah, Takahiro Okumurai, Yuichi Babaj, and Tohru Minaminoa,k |
| Title of original paper | Clinical characteristics and prognosis of patients with isolated cardiac sarcoidosis: Insights from the ILLUMINATE-CS study |
| Journal | European Journal of Heart Failure |
| DOI | 10.1002/ejhf.3056 |
| Affiliations | a Department of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine b Department of Cardiology, Kameda Medical Center c Department of Cardiovascular Medicine, Kitasato University School of Medicine d Department of Cardiology, Leiden University Medical Center e Division of Cardiology, Internal Medicine III, Hamamatsu University School of Medicine f Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center g Department of Cardiovascular Medicine, Osaka University Graduate School of Medicine h Division of Cardiovascular Medicine, Department of Internal Medicine, Kobe University Graduate School of Medicine i Department of Cardiology, Nagoya University Graduate School of Medicine j Department of Cardiology and Geriatrics, Kochi Medical School, Kochi University k Japan Agency for Medical Research and Development-Core Research for Evolutionary Medical Science and Technology (AMED-CREST), Japan Agency for Medical Research and Development |